
My quest to understand vitamins has taken some interesting turns. Two weeks ago, I learned that whether a vitamin is natural or synthetic is not important. The importance relates to a vitamer’s bioavailability and biopotency. It became clear that vitamins have more immediate missions than preventing deficiency diseases. This week, the third in a series of four, I turn my attention to vitamin bioavailability and toxicity. Next week I will discuss biopotency. Vitamins A and D illustrate my points this week. My guidebook on this journey is the latest edition of The Vitamins by Combs and McClung.

The next two questions follow:
5.What is bioavailability and how does it apply to the nutritional value of vitamins? Food scientists obsess about bioavailability of vitamins and minerals. When adding a vitamer to a food formulation, product developers want to know many things. First, does it have any adverse effects on flavor, color, or texture? Many added vitamins add off-flavors to foods. This property presents a critical challenge to the developer. Next, comes bioavailability of the nutrient at a given cost. It is not only the amount of a vitamin added but its ability to get to the target in the body and its performance. Vitamin stability is also important. How will it withstand processing and storage after processing? A shelf-life study could be necessary to ensure the vitamin is present at end of shelf life. A claim like “a good source of vitamin X” would involve consultation with a legal team. This action ensures the content of the food product supports the claim. *
Bioavailability of a vitamin involves its accessibility within the food matrix. It also includes absorption in the gut. Note, the vitamin must be stable in the food. Vitamins in raw fruits and vegetables are susceptible to biochemical degradation. Food processing that involves heat, light, or oxygen also degrades vitamins. During digestion, bioavailability depends on freeing the vitamin from the matrix. Then the vitamin must cross the intestinal mucosa into the bloodstream. If the vitamin stays in the gut, it is useless to the body. Bioavailability also incorporates ‘biopotency.’ The authors use this term instead of ‘nutritional value’. Biopotency refers to the effectiveness of the vitamer at the site in the body.
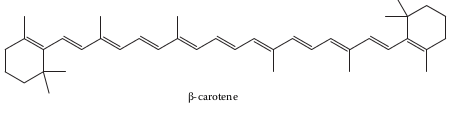
I select vitamin A to illustrate bioavailability and biopotency. First, β-carotene is the form of vitamin A most of us consume. β-carotene is one of many plant carotenoids with provitamin A potential. β-carotene breaks down into retinal and retinol, two molecules with vitamin A activity. Other retinyl esters are also active. We find such retinyl esters in animal fat, dairy products, eggs, and meats. Carotenoids function as orange, red, and yellow pigments in fruits and vegetables.
Vitamin A is active in human metabolism. Its vitamers provide visual pigments in cones of the eye helping us to see different colors. The vitamin acts like a hormone to regulate gene activity for glucose metabolism. It may regulate insulin synthesis and aid in weight loss. Carotenoids and vitamin A protect cells from free radicals that lead to oxidation. The vitamin helps protect the immune system, vascular development and skin health.
Deficiency of vitamin A accompanies low levels of zinc and other nutrients. Early clinical signs of vitamin A deficiency focus on eye health. Night blindness and permanent changes in eye shape can lead to total blindness. Low serum retinol is a threat to children and pregnant women. High-dose supplementation reverses the disease in children. Low-dose supplementation protects vulnerable populations from developing a deficiency. Recent approval of Golden Rice in Asia may help prevent vitamin A deficiency in the threatened population. It is not clear how a funny-looking grain will be acceptable to traditional rice consumers. Carotenoids may impart off-flavors into the rice. Healthy foods are not beneficial if they are not consumed.
Bioavailability of vitamin A depends on many factors. Carotenoids occur in chromoplasts and chloroplasts of plant tissue. Chloroplasts bind carotenoids more than chromoplasts in the digestive tract. Thus, orange fruits and vegetables release more β-carotene in the gut than leafy greens. Cooking helps release the provitamin. Cooked and processed fruits and vegetables are better sources than their raw counterparts. Absorption of fat-soluble vitamins like vitamin A improves with higher-fat meals. Uptake of carotenoids into target cells occurs by facilitated diffusion. The level of the vitamin A in mucosa affects absorption. It is in the mucosa that β-carotene splits to form retinal and retinol. Vitamers travel to the liver and stored until needed in other locations. Transport from the liver occurs via low-density lipoproteins (LDLs), aka the “bad” cholesterol.
Like most fat-soluble vitamins, too much vitamin A can be toxic. It may be the most toxic vitamin. The biggest problem with toxicity of this vitamin is overdosing. Too much of the vitamin occurs by either a one-time dose or too much of the vitamin taken daily. As with too little vitamin A, hypervitaminosis leads to eye damage. Acute toxicity elicits many symptoms including abdominal pain, blurred vision, headache, and nausea. Chronic toxicity of the vitamin can lead to alopecia, diarrhea, and insomnia.
6.What are the consequences of consuming too much of a single vitamin? Food scientists also obsess over vitamin toxicity. Dietitians, nutritionists, and food scientists prefer us to get our vitamins from food. Dietitians and nutritionists favor vitamins from whole foods. Food scientists consider processed foods to be valid sources as well. Either way it can be a delicate balance. Relying on a small number of foods, whole or processed, risks not enough of some vitamins and too much of others. As long as we maintain adequate stores of each vitamin without excess levels of others, we should be good. As noted last week, we can’t know without bloodwork.
A generality about toxicity of vitamins is that water-soluble vitamins don’t accumulate. Fat soluble-vitamins do. Thus, fat-soluble vitamins are more likely than water-soluble vitamins to become toxic. Like many generalities about vitamins, this one has exceptions as well. Fat-soluble vitamin A has protective mechanisms to decrease the chances of hypervitaminosis. Water-soluble ascorbic acid and niacin can be toxic at higher levels than needed. Hypervitaminosis comes in two forms: acute and chronic. Acute cases come from consumption of a single high dose. Chronic exposure results from lower doses exceeding dangerous levels over longer periods.
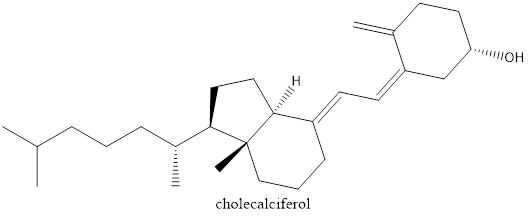
Vitamin D is another fat-soluble vitamin that can be toxic when consumed at high levels. Symptoms of chronic exposure include diarrhea, drowsiness, frequent urination, and vomiting. Excess levels of the vitamin can lead to loss of calcium in bones. Increased susceptibility to fractures can also occur. Vitamin D3 is more bioavailable and thus more toxic than vitamin D2.
Physiological functions of vitamin D include regulation of calcium and phosphorus metabolism. The vitamin’s main target is bone, but it also affects soft tissue. It is important in digestive, fat-cell, immune, and muscle functions. Vitamin D contributes to cardiovascular, nerve, pregnancy, and skin health. It is the only vitamin that is available by exposure to sunlight.
The classic Vitamin D deficiency disease is rickets. Symptoms include severe malformation of bones. Children under five years old are most affected. Older children and adults suffer from osteomalacia (bone softening) or osteoporosis (porous bones). Subclinical effects include greater susceptibility to inflammatory bowel disease, tuberculosis, and viral diseases.
A recent study (1) sent shockwaves through the vitamin D-research community. The main conclusion of the study was that
“Vitamin D3 supplementation did not result in a significantly lower risk of fractures than placebo among generally healthy midlife and older adults who were not selected for vitamin D deficiency, low bone mass, or osteoporosis.”
An accompanying editorial (2) recommended
“that providers should stop screening for 25-hydroxyvitamin D levels or recommending vitamin D supplements, and people should stop taking vitamin D supplements to prevent major diseases or extend life.”
It is clear that vitamin D tablets are not magic pills. No vitamin supplement comes as a magic pill. The only diseases cured or prevented by vitamins are the specific deficiency diseases. Osteoporosis results from impaired vitamin D metabolism. It also involves calcium and phosphorous. More research the roles of all should focus on other potential preventative measures. The study (1) looked at fractures and not conditions of osteoporosis or osteomalacia. Subjects were “healthy midlife and older adults.” They were not screened for conditions associated with vitamin D insufficiency. The commentary (2) highlights the importance of the study. Those authors appear to have overstated their recommendations to physicians.
Take-home lesson. It is not how much of a vitamin we consume that counts. It is how bioavailable it is that affects our health. The % Daily Value on a product label takes some of that information into account. Stability of the vitamin in the food can decrease the amount of a vitamin. Variability between individual persons affects absorption. We need to understand that hypervitaminosis is real and can be unhealthy. Vitamins A and D are the most toxic vitamins. Acute or chronic exposures are unhealthy. A multivitamin tablet can provide some personal assurance. Further supplementation without oversight by a medical professional is risky.
What I have learned to this point in my quest is that there is a golden mean of vitamin intake. For most of us it is not about the deficiency disease for a specific vitamin. It is about maintaining adequate stores over time. Not enough and our metabolism suffers and susceptibility to chronic disease increases. Too much can become toxic. Finding the appropriate balance is not easy. For me this post was personal. Two decades ago I received a diagnosis of osteopenia (a milder form of osteoporosis). My physician prescribed Fosamax. It did not seem to help me, and he discontinued the prescription. Two weeks ago, I had in a minor bike accident. During my fall, I cracked a rib. My symptoms are mild and my pain is subsiding. It is an odd confluence of events for a post planned months ago. Vitamin D pills would have offered me little or no protection from cracking my rib.
*Thanks to Christine Addington and Karen Penichter. They helped on the role of a product developer in vitamin addition to processed products.
Next week: Vitamin biopotency
References:
(1) LeBoff, MS, S Chou, KA Ratliff, NR Cook, B Kurana, E Kim, PM Cawthon, DC Bauer, D Black, JC Gallagher, I-M Lee, JE Buring, and JE Manson, 2022. Supplemental Vitamin D and incident fractures in midlife and older adults. N Engl J Med 387:299-309. DOI 10.1056/NEJMoa2202106
(2) Cummings, SR and C Rosen, 2022. VITAL findings—a decisive verdict on vitamin D supplementation. N Engl J Med 387:368-370.

As one of those dietitians who prefer to get my vitamins from food, I don’t even take a multivitamin. When I worked in a Manhattan based fitness club, I love to use the analogy of the health food store. Vitamins are arranged in alphabetic order which made it much easier to find and gave the process the aura of certainty. But I would explain it was a false sense of security. Same in my opinion for the % Daily Value on a product label. Both project certainty but I would argue, it’s a false sense of certainty. Without bloodwork and individual bioavailability, it’s at best second guessing. Maybe it helps. Hopefully does no harm. Can make for expensive urine. Nutrition is wicked hard.
LikeLike
As a food scientist who considers processed food as valid sources of vitamins, I do not take supplements either. I agree with you that there is no certainty in Nutrition. That doesn’t mean that we should ignore science. Science is a guide not a guarantee. Information helps us make choices. Critics of processed foods would have us believe that these products have no nutritional value at all. As far as expensive urine, I used to tell that to my students in classes. It turns out that not all water-soluble vitamins are excreted in the urine when consumed in excess. From the book I was surprised to learn that very little ascorbic acid goes out in the urine.
LikeLike